
Coughing is one of the most common presenting complaints for dogs in small animal practices. The clinical signs associated with coughing may present a diagnostic challenge to the practitioner as the cough in some animals is clinically less significant and/or self limiting, while in others it may be far more serious. Furthermore, clients may often confuse a cough with a gag, wheeze, labored breathing, or a reverse sneeze; and some dogs may retch or vomit after coughing which may be misinterpreted as gastrointestinal disease.
A plethora of disorders can result in a cough, with etiologies ranging from cardiovascular disorders, degenerative disorders, parasitic disease/burden, allergic states, physical causes/trauma, inflammation and/or neoplasia.
A thorough patient history and clinical examination are essential in planning the optimal diagnostic workup which will often include radiology. In this article, we will review some of the common radiographic lung patterns and distributions identified in coughing dogs while putting the clinical picture together.
History and Clinical findings:
By integrating the patient's history, signalment and physical exam findings along with the radiographic pattern and distribution, one can often narrow down the differential list and ultimately the cause of coughing.
Younger animals or those exposed to other dogs (eg. shelter, boarding facilities) are more prone to developing a cough due to infectious etiology, while parts of the country lived in and/or traveled to influence the likelihood of other diseases like heartworm disease or fungal infections (histoplasmosis, coccidioidomycosis and blastomycosis).
With respect to breed and age; middle aged to older, small breed dogs are more likely to have valvular heart disease while middle aged to older, large breed dogs are more likely to develop laryngeal paralysis. Tracheal collapse also occurs most commonly in middle aged overweight small breeds. In older patients, neoplastic causes need to be considered.
When the cough occurs might also be significant. Coughs which occur more frequently at night may be suggestive of cardiogenic pulmonary edema and/or tracheal collapse. In other instances, it might frequently occur following excitement or when pressure is placed around the tracheal area. Coughing associated with eating and/or drinking may be suggestive of laryngeal/pharyngeal disorders.
Descriptors may also be helpful for localizing airway pathology or suggesting cough etiology. Productive coughs are typically moist and low pitched and suggest accumulation of fluid in the airways (eg. pneumonia, edema), while non-productive coughs are dry, harsh and high pitched/honking (eg. airway collapse, chronic bronchitis). It is worth noting that while expectoration of mucus from the trachea into the pharynx typically occurs with productive coughs, most owners do not recognize a productive cough as animals often swallow the expectorated material. If hemoptysis is described/observed, coagulopathy, neoplasia, severe heartworm and pneumonia need to be considered. It is important to be mindful of pneumonia in patients that have been vomiting, undergoing anesthesia, prolonged recumbency, have megaesophagus, immune compromise and/or airway susceptibility.
Physical examination findings are also pertinent to the diagnostic workup. Crackles during thoracic auscultation may suggest pulmonary edema, pneumonia, bronchial collapse and/or pulmonary fibrosis, while wheezing is usually characteristic of chronic bronchitis and dull respiratory sounds usually suggest pathology of the pleura or within the pleural space (pleural effusion, pneumothorax, intrathoracic masses, diaphragmatic hernias etc). Lastly, increased inspiratory effort is suggestive of extrathoracic airway disease, while increased expiratory effort is suggestive of intrathoracic airway disease.
Radiology:
The radiographic pattern and distribution of changes are often helpful for prioritizing differential diagnoses for coughing in canines.
While evaluation of the heart, pulmonary vessels and pulmonary parenchyma is necessary, this article will focus on the evaluation of the pulmonary parenchyma with brief overviews of the pattern-based-approach and the distribution of lesions which has recently received more emphasis with regard to the differential list.
Common lung patterns include:
Interstitial patterns indicate disease or disruption of the interstitium. Characteristic findings include an increased opacity in the lungs that partially obscures blood vessel margins, which may be due to the presence of edema, pus, blood or other material in the lungs. Interstitial patterns are classified as either unstructured or structured. The distribution of unstructured interstitial patterns is more suggestive of certain differentials than the appearance of the pattern itself and most commonly include, pulmonary edema, pneumonia, pulmonary thromboembolism (PTE), hemorrhage and/or fibrosis. Differentials for structured/nodular (round or ovoid soft tissue opacities) insteritial patterns include neoplasia, fungal disease, parasitic cysts, bulla, pulmonary osteomas and granulomas.
An alveolar pattern is more severe than an interstitial pattern where the increased opacity in the lungs completely obscures the blood vessel margins. Air bronchograms and lobar signs may also be present. Differential diagnoses for alveolar patterns are similar to those for interstitial patterns.
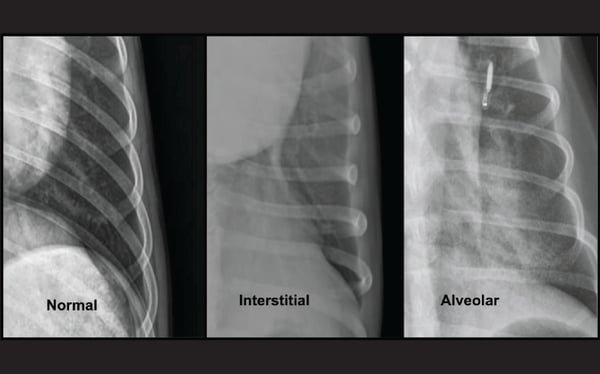
Magnified images of the left caudal lung field in three separate dogs demonstrating the various extent to which the pulmonary vessels are obscured by the increased pulmonary opacity in interstitial and alveolar patterns respectively. With interstitial patterns the pulmonary vessels are still visible, but have hazy margins (“trees in the fog” appearance), in contrast to alveolar patterns where the vessel definition is completely obscured (air bronchograms may or may not be present).
Bronchial patterns are distinct from interstitial and alveolar patterns, with thickening of the larger, conducting airways. The radiographic effects are ring-like opacities (“donuts”) and parallel lines (“tram lines”), which stand out from the interstitium. Sometimes peribronchial cuffing (indistinct opacities surrounding the airway) exacerbates the bronchial pattern. The primary differentials for a true bronchial pattern include chronic lower airway disease of allergic (chronic bronchitis), infectious (Canine infectious respiratory disease complex - CIRDC) or parasitic (e.g. Dirofilaria immitis/heartworm) etiology.
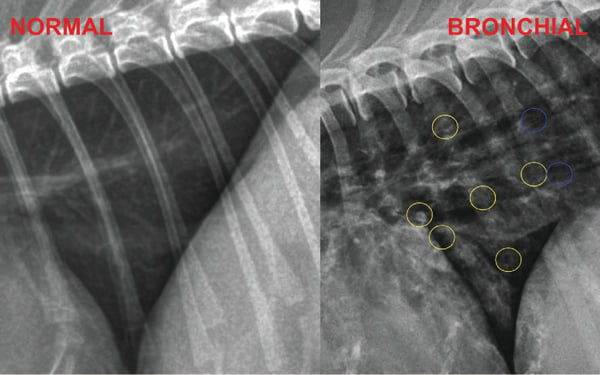
Bronchial patterns are distinct from interstitial and alveolar patterns, with diffuse thickening of the airway walls giving rise to thickened ring-like opacities (“donuts''; yellow circles) and parallel lines (“tramlines”; blue circles). A distinction between alveolar/interstitial patterns and bronchial patterns should be made, since each is unique to a certain subset of diseases. While bronchial signs may be a normal variant in senior patients, age related bronchial mineralisation leads to distinct, thin walled bronchial opacities in comparison to the thicker, slightly indistinct bronchial opacities in a true bronchial pattern.
Vascular patterns are when enlarged and/or tortuous vessels become evident in the lungs with differentials mostly limited to heartworm disease, left sided congestive heart failure, or left to right sided cardiac shunts.
Radiographic distribution of pulmonary patterns:
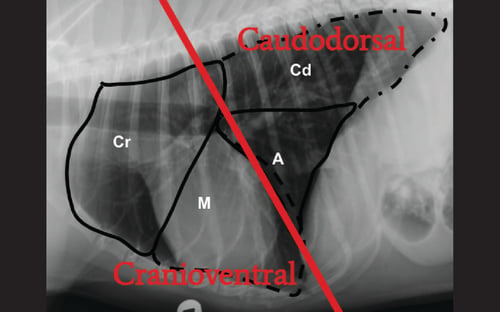
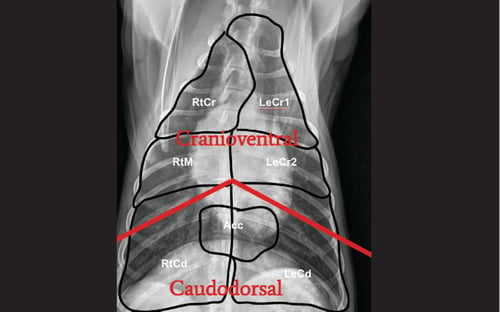
Recently more emphasis has been given to the distribution and appearance of lesions than to the pattern alone. These include:
Cranioventral Distribution: Differential diagnoses for alveolar patterns and interstitial patterns are mostly the same. When either pattern occurs with a cranioventral distribution, most common differential diagnoses include aspiration pneumonia, atelectasis, hemorrhage, thromboembolism, lung lobe torsion, abscesses and masses.

Caudodorsal Distribution: Interstitial to alveolar patterns with a caudodorsal distribution include a different subset of diseases which include cardiogenic and noncardiogenic pulmonary edema, hematogenous, viral or atypical pneumonias, pulmonary contusions, PTE and neoplasia. It should be noted that there is no difference in the distribution of cardiogenic and noncardiogenic pulmonary edema, the only difference being the presence/absence of pulmonary venous enlargement and/or cardiomegaly.
Caudal lobar alveolar patterns are unique to foreign body-associated pneumonia, and less commonly alveolar cell carcinomas.

Diffuse patterns: Diffuse patterns may be in the form of a bronchial pattern (see above), or diffuse interstitial or alveolar pattern.
- Diffuse bronchial patterns: These may be due to infections or inflammatory airway disease (e.g chronic bronchitis, eosinophilic bronchopneumopathy {EBP}, infectious bronchitis by Mycoplasma or Bordetella).
- Canine infectious respiratory disease complex (CIRDC) or Kennel Cough is a common cause for diffuse bronchial patterns in young dogs and dogs with a history of exposure to a shelter or boarding facility. There may/may not also be concurrent aspiration pneumonia. Mycoplasma testing should be carried out in patients which do not respond to treatment after 7 days.
- Dogs with EBP will often show an alveolar component in addition to the bronchial pattern on thoracic radiographs. It's worth noting that in contrast to dogs with chronic bronchitis which are systemically healthy, dogs with EBP are systemically unwell. Furthermore, approx. 50% of these dogs will also have a chronic nasal discharge and peripheral eosinophilia.
- Diffuse interstitial or alveolar patterns: These may be due to vasculitis, acute lung injury (ALI), acute respiratory distress syndrome (ARDS), atypical pneumonia or neoplasia.

Other radiographic findings:
Miliary patterns: These are common in fungal pneumonias and neoplasia.

Perihilar lymphadenopathy: These are common in fungal pneumonia, neoplasia and EBP.

Narrowed trachea and/or bronchi: Suggestive of airway collapse (tracheomalacia and/or bronchomalacia, respectively).

Conclusion
We hope the tips offered in this brief overview help you better understand the types of patterns and their distributions as well as their possible causes. Considerations should be given to the various differential diagnoses before selecting diagnostic tests and planning appropriate treatment.
If you’re interested in learning more about coughing in dogs, and receive 1-hour RACE approved CE, you can register for our on-demand webinar, “The Coughing Dogs: Is it Cardiac or Respiratory?”
